AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2640-1045/054
1 Department of Internal Medicine, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria.
2 Department of Nursing Science, College of Health Sciences / School of Postgraduate Studies, Nnamdi Azikiwe University Awka, Nnewi Campus, Anambra State, Nigeria.
3 Department of Internal Medicine, Federal Medical Centre, Owerri, Imo State, Nigeria.
4 Department of Internal Medicine, Ahmadu Bello University Teaching Hospital, Zaria, Kaduna State, Nigeria.
*Corresponding Author: Chidiebele M. Ezeude, Department of Internal Medicine, Endocrinology, Diabetes and Metabolism Unit, Nnamdi Azikiwe University Teaching Hospital, P.M.B 5021, Nnewi. Anambra State, Nigeria.
Citation: Chidiebele M. Ezeude, Afoma M. Ezeude, Anthony C. Anyanwu, Ogonna C. Oguejiofor, Henry M. Nwankwo, Adamu G. Bakari (2020) Erectile Dysfunction in a Cohort of Eugonodal Type 2 Diabetic Men Attending a Tertiary Healthcare Facility: Prevalence and Correlation with Testicular Volume J. Endo and Dis; 4(1); DOI:10.31579/2640-1045/054
Copyright: © 2020, Chidiebele M. Ezeude, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 September 2020 | Accepted: 05 October 2020 | Published: 26 November 2020
Keywords: erectile dysfunction; type 2 diabetes mellitus; eugonadal; hypogonadism; testicular volume; Prader orchidometer
Background: Erectile dysfunction (ED) is a very common complication of diabetes mellitus. The prevalence of ED in diabetic patients, especially those with type 2 diabetes mellitus (T2DM) is very high compared with their non-diabetic counterparts. There are few studies on ED and its correlation with testicular volume in eugonadal type 2 diabetics globally and especially in sub-Saharan Africa.
Objective: To access the prevalence and correlation of ED with testicular volume in T2DM patients attending the diabetes outpatient clinic of Nnamdi Azikiwe University Teaching Hospital, Nnewi in South-eastern Nigeria.
Materials and Methods: This was a cross sectional prevalence study comprising 124 subjects with T2DM and 62 non diabetic controls. Data collection was done using a study protocol. Hospital Anxiety and Depression Scale (HADS) and the International Index of Erectile function (IIEF) questionnaires were used for diagnosis of anxiety/depression and erectile dysfunction respectively. Testicular volumes for the study subjects were estimated using Prader-orchidometer. Serum total testosterone, follicle stimulating hormone and luteinizing hormone levels were determined. Participants who had anxiety, depression or hypogonadism were excluded from the study. Statistical analysis was done using Statistical Package for Social Sciences (SPSS) version 20.
Results: The mean age of the subjects was 58.29 ± 10.02 while that of the controls was 56.48 ± 10.58 (P = 0.255). 48.4% of the subjects had ED while 4.8% of the controls had erectile dysfunction (P < 0.001). Of the subjects that had ED, 26.7% had mild, 11.7% had moderate while 61.7% had severe erectile dysfunction. Severe ED was more associated with subjects (χ2= 7.230, P = 0.027). IIEF score has significant positive correlation with the mean testicular volume.
Conclusion: Prevalence of ED in men with T2DM in Nigeria is high and there is a significant positive correlation between ED and testicular volume in this group of subjects.
Erectile function is dependent on relaxation of the cavernous smooth muscle and its mechanism of action is mediated by nitric oxide (NO) [1]. Vasoconstrictions maintain the penis in the flaccid state.
Erectile dysfunction (ED) on the other hand is a persistent inability to achieve or maintain penile erection for satisfactory sexual intercourse [2]. It is one of the chronic complications of diabetes mellitus.
The causes of erectile dysfunction fall into two main categories: organic and psychogenic [3]. Idiopathic and familial causes of ED are also encountered in clinical practice [4].
The key pathophysiologic mechanisms for ED revolve around organic (mainly vasculopathy and neuropathy) and psychogenic mechanisms (especially anxiety and depression) [3]. Diabetes causes ED mainly by causing vasculopathy and neuropathy. At Uyo, Niger Delta, Nigeria a study showed that 7.3% of cases of ED resulted from diabetes mellitus [5].
The burden of ED in subjects with DM, especially type 2 DM is set to increase in the future since ED was found to precede the diagnosis of type 2 DM in 36.3% of cases [6]. Diabetes mellitus is assuming a pandemic level globally. International Diabetes Federation (IDF) estimated that 425 million people had DM globally and that this figure is projected to rise to 629 million by the year 2045 [7]. Type 2 diabetes makes up about 90.0% of the cases of diabetes mellitus [8]. The predominant age of occurrence of DM is 40-59 years and worldwide estimate projects that in 2030 the greatest number of individuals with DM will be aged 45-65 years [9]. These are age ranges during which most men are sexually active and father children.
Erectile dysfunction in the setting of type 2 DM is associated with a negative impact on emotional wellbeing and poor quality of life (QOL) [10]. There is increasing evidence that ED is a risk factor for cardiovascular diseases and early marker for coronary artery disease, which is the leading cause of mortality in patients with diabetes mellitus [11]. This is consistent with the inactivation of the anti-aging gene, Sirtuin-1. Sirtuin-1 repression is connected to the development of cardiovascular diseases and type 2 diabetes. It is equally connected to the development of ED, and treatments that activate Sirtuin-1, reverse ED in experimental rats [12].
The prevalence rate of ED among the general population in Nigeria was 19.8% [13], while that among type 2 DM patients was 87.8% and 71.1%1 [14,15]. The prevalence rate of ED in subjects with type 2 DM was 67.9% in Ghana [16].
The prevalence of ED in patients with type 1 DM reported by Fedele et al and Maiorino et al was 26% and 37% respectively [17,18].
The high prevalence of ED in men with diabetes underscores the need for an early diagnosis and treatment of this worrisome condition in this group of patients. The effective medical treatment of ED generally involves the use of the oral agent: phosphodiesterase type 5 (PDE5) inhibitors like sildenafil, tadalafil and vardenafil. The PDE5 is the primary phosphodiesterase in cavernosal smooth muscle responsible for degradation of cyclic guanosine monophosphate (cGMP) and its inhibitors are the first line agents in the treatment of erectile dysfunction [19]. Testosterone replacement therapy is also indicated in men with ED and concomitant hypogonadism. Recent guideline recommends testosterone supplementation for symptomatic men with morning total testosterone below 8 nmol/L [20]. The application of gene therapy as a viable treatment option for ED and other chronic pathological conditions appears promising in preclinical trials but the therapeutic approach still requires clinical studies in humans [21]. Yu et al found that resveratrol, an activator of Sirtuin-1 restores erectile function while Sahan et al noted that Melatonin, via Sirtuin-1 expression prevents deterioration of erectile function in streptozotocin-induced diabetic rats respectively [22,23].
There is paucity of available data on erectile dysfunction in type 2 DM subjects with normal total testosterone levels both locally and globally. Most studies done on the prevalence of ED in T2DM patients did not exclude hypogonadal subjects and this could have falsely increased the prevalence rates of type 2 diabetes-induced ED from these studies. The reason is that hypogonadism, having several other causes other than T2DM is clearly associated with increased prevalence of ED because testosterone plays a major role in penile erection.
Also, to the best of our knowledge there is no published study in the sub-Saharan Africa that evaluated the correlation between ED and testicular volume among eugonadal T2DM subjects. Equally, studies have also shown that clinicians do not enquire about sexual dysfunction during diabetes consultations and that there is low prevalence of self-reported erectile dysfunction usually owing to the social stigma attached to it [24]. These made ED one of the most undiagnosed and yet treatable complications of diabetes mellitus. This study was aimed at addressing these gaps in knowledge, as well as answering these questions: is there a difference in the frequency of occurrence of ED in type 2 DM subjects, when compared with their non diabetic counterparts? Is there a correlation between ED (IIEF score) and testicular volume among T2DM subjects with normal serum total testosterone levels?
Research design
This was a cross sectional hospital-based prevalence study comprising 124 subjects with type 2 DM and a control group of 62 non diabetic subjects. All the study participants were classified based on their age into three groups: young, middle aged and elderly. Young age was taken as 18-44 years, middle age as 45-64 years and old age as 65 years and above [25].
Study site and study population
This study was carried out at the diabetes clinic of the Department of Internal Medicine of Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi, in Anambra State, south-eastern Nigeria. Nnewi is one of the major towns in Anambra State, and is well known for her industrial and commercial activities.
Nnamdi Azikiwe University Teaching Hospital, Nnewi is the major tertiary health center in Anambra State and serves the entire state and parts of the neighboring states of Imo, Delta, Enugu, Ebonyi and Abia states.
The study population consisted of consenting male T2DM patients aged 30 years and above who presented consecutively to the NAUTH diabetes clinic for treatment. Age and sex-matched control subjects without diabetes were recruited from medical out-patient clinic for this study.
Exclusion criteria for the subjects included type 1 DM, a history of pelvic/penile trauma or surgery, psychiatric illness or antipsychotic medication use, hypogonadism, unfavourable penile anatomy for sexual act, urinary tract infection or severe illness including clinical finding of or history of cardiac disease. Those of the controls in addition, included diabetes mellitus or impaired fasting glucose [26].
Ethical clearance for the study was obtained from the ethical committee of the Nnamdi Azikiwe University Teaching Hospital, Nnewi and written informed consent was gotten from all the study participants.
Data collection and procedure
A total of 246 study participants were recruited at the beginning of this study. They comprised 172 subjects with type 2 DM and 74 non diabetic controls. All the study participants were met individually by the primary investigator as they presented consecutively at the diabetes and the endocrine clinic respectively. Written consent was obtained from all the study participants. Each participant filled in the Hospital Anxiety and Depression Scale (HADS) questionnaire for the diagnosis of anxiety and depression [27]. The history of the use of antipsychotic drugs was obtained from all the participants [26]. None of the diabetic subjects and the controls had anxiety or depression and none was on antipsychotic medication.
The participants were scheduled by to come to the medical ward side laboratory between 8a.m and 9a.m on the appointed day, following an overnight fast of 8-14 hours and venous blood samples were drawn for fasting plasma glucose (FPG), serum total testosterone, follicle stimulating hormone (FSH) and luteinizing hormone (LH) assays. Also, the International Index of Erectile Function (IIEF) questionnaire was administered to all the study subjects [28]. The contents of both the IIEF and HADS questionnaires were translated into the local language (Igbo) for those who were not proficient in English language and their responses were filled in appropriately. The IIEF questionnaire and serum total testosterone were used for diagnosing erectile dysfunction and hypogonadism respectively [26]. A focused history was obtained and a detailed physical examination, including urogenital examination was done. Testicular volume (size) for each testis was estimated in mL for the T2DM subjects using Prader-orchidometer and the mean testicular volume calculated [29]. Erectile dysfunction was taken as a score of ≤ 25 in the IIEF questionnaire: mild ED was a score of 17-25, moderate ED was 11-16 and severe ED was a score 6-10 in IIEF questionnaire [28]. Hypogonadism was taken as morning serum total testosterone level < 280ng>
A total of 48 (27.90%) type 2 DM subjects had low serum testosterone level and were excluded from further participation in the study [26]. Similarly, 10 (13.51%) non diabetic subjects had hypogonadism and were equally excluded from further participation in the study, while 2 declined further participation in the study. Overall, 124 type 2 DM subjects and their 62 non diabetic counterparts concluded the study.
Statistical analysis
Statistical analysis was performed using SPSS version 20 (SPSS Inc. Chicago, Illinois, USA). Descriptive statistics, which include frequency, percentages, means and standard deviation were used to summarize categorical and continuous variables. Associations between categorical variables were done using Chi square test and logistic regression. Student’s t-test was used to compare means of continuous variables. Level of significance was set at P < 0>
A total of one hundred and eighty-six (186) subjects met the inclusion criteria and were studied. One hundred and twenty-four (124) of them had type 2 diabetes mellitus (subjects) while sixty-two (62) did not have diabetes mellitus (controls).
Descriptive statistics
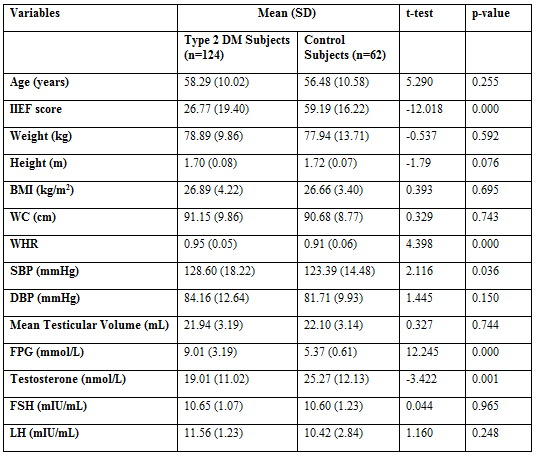
Table 1 shows the descriptive statistics of base line characteristics in both type 2DM subjects and controls. Waist hip ratio (WHR), systolic blood pressure (SBP) and fasting plasma glucose (FPG) were significantly higher in subjects with type 2 DM compared with controls while IIEF score and serum Testosterone levels were significantly higher in control subjects compared with their counterparts with type 2 diabetes mellitus.
Prevalence of erectile dysfunction in subjects and controls
Table 2 shows that 60 (48.4%) of the subjects had erectile dysfunction while 3 (4.8%) of the controls had erectile dysfunction. Erectile dysfunction was significantly associated with subjects with type 2 diabetes (P < 0 xss=removed xss=removed>

Age distribution of subjects and controls
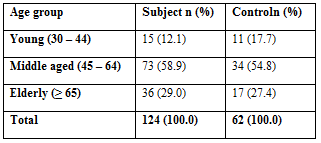
Table 3 shows that of the 124 subjects studied, 15 (12.1%) were young, 73(58.9%) were of middle age and 36 (29.0%) were elderly. For the controls 11(17.7%) were young, 34 (54.8%) were of middle age and 17 (27.4%) were elderly. There was no statistically significant difference between the different age groups in both the subjects and controls (χ2 = 1.097, P = 0.578).
Table 4 shows that the mean age of the subjects was 58.29 ±10.02 while that of the controls was 56.48 ± 10.58 (P = 0.255). The difference was not statistically significant.

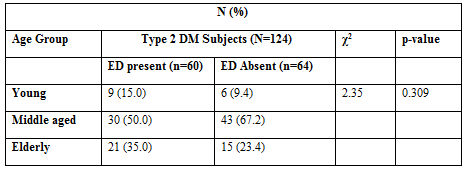
Prevalence of erectile dysfunction among the various age groups in the subjects
Table 5 shows that more individuals in the young and elderly age groups
had ED compared with those without ED, although this was not statistically significant (P= 0.309). Reverse was the case with the middle age group as those without ED were more than those that had erectile dysfunction. This was equally not statistically significant (P= 0.309).
Degree of erectile dysfunction among subjects and controls
Table 6 shows that out of 60 subjects with erectile dysfunction, 16 (26.7%) had mild, 7 (11.7%) had moderate while 37 (61.7%) had severe erectile dysfunction. In the same vein, out of 3 controls with erectile dysfunction, none had mild, 2 (66.7%) had moderate while 1 (33.3%) had severe erectile dysfunction. Severe erectile dysfunction was more associated with the subjects (χ2 = 7.230, P = 0.027).

Mean comparison of age between subjects and controls with and without erectile dysfunction
Subjects with erectile dysfunction were significantly older, with mean age of 61.00 ± 10.79 when compared with those without erectile dysfunction with mean age of 55.77 ± 8.55; (t = 3.002, P = 0.003).
Controls with erectile dysfunction had a significantly higher mean age of 73.00 ± 3.46 when compared with that of those without erectile dysfunction with mean age of 55.64 ± 10.13 (t = 2.939, P = 0.005).
Correlation of IIEF score with mean testicular volume, serum testosterone, FSH and LH concentrations among type 2 diabetic subjects
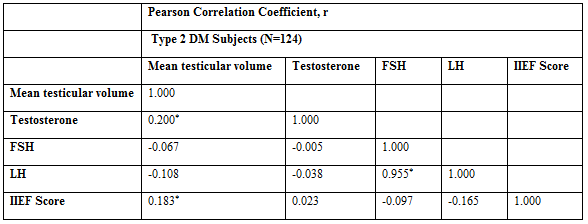
Table 7 shows the correlation of IIEF score with mean testicular volume, serum testosterone, FSH and LH in the study subjects with type 2 diabetes mellitus. International Index of Erectile Function score positively correlated with each of mean testicular volume and serum testosterone but negatively correlated with each of serum FSH and LH. The association of IIEF score with mean testicular volume was the strongest and this relationship was statistically significant.
Prevalence of erectile dysfunction in patients with type 2 diabetes mellitus
This was a cross sectional hospital-based study which aimed at assessing the prevalence, pattern and correlation of erectile dysfunction with testicular volume in subjects with type 2 diabetes mellitus. Non diabetic controls were also studied and compared with the subjects with type 2 diabetes mellitus.
This study showed that the prevalence of ED among subjects with T2DM was 48.4% while that of the non-diabetic controls was 4.8% (P < 0 xss=removed xss=removed>
In this study, ED is about eighteen times more likely to occur in type 2 diabetic subjects compared to their non diabetic counterparts. This significant association between ED and type 2 DM re-emphasizes an already established fact. The prevalence of ED in type 2 DM subjects from this study is lower than what was observed in studies of ED in type 2 diabetes in other parts of Nigeria. For example, a prevalence of 87.8% was reported in Jos and 71.1% in Ile-Ife [14, 15]. Also, the prevalence of ED in diabetic subjects was 72.7% in Ibadan [33]. These other studies equally had middle aged and elderly men among their study participants, but unlike this study, did not exclude subjects who had low testosterone level and this could account for the wide margin between the prevalence of ED in this study and their own. This is in view of the fact that aging men are prone to hypogonadism, causing age-induced erectile dysfunction [34].
It is also possible that this study by excluding all subjects with hypogonadism, also excluded some young and middle-aged men who may have had ED resulting from type 2 DM induced hypogonadism [35]. This is in view of the fact that Ogbera et al reported that the prevalence of symptomatic hypogonadism in subjects with type 2 DM in Lagos, Nigeria was 36.0% [36].
The study done in Jos in addition had a small sample size of 66 [14]. The mean age of their subjects as 56.0±8.8 [14] and is comparable to that of this study (58.29±10.02 years). Similarly, Adebusoye et al in Ibadan studied only 33 diabetic subjects [33]. The small sample sizes could also account for the higher prevalence rates reported by these studies.
The prevalence rate of erectile dysfunction in type 2 DM subjects in Ghana was 67.9% [16]. This study equally did not exclude type 2 DM subjects with hypogonadism.
Higher prevalence rates of ED in type 2 DM subjects were also found in Italy (60.0%) and Iran (59.5%) [31, 32]. These studies did not exclude type 2 DM subjects who had low serum testosterone levels.
An equally plausible reason for the lower prevalence of ED from our study could be from the fact that many of our type 2 DM subjects were equally hypertensive. Most of study subjects were on angiotensin receptor blockers (ARBs), angiotensin converting enzyme inhibitors (ACE-Is) and or calcium channel blockers (CCBs) either as antihypertensive or anti-proteinuric medication. Angiotensin receptor blockers had been reported in a study to exhibit a beneficial effect on erectile function while CCBs and ACE-Is seemed to have neutral effect [37].
Another possible reason for the higher prevalence rates in these studies could be due to the differences in methodology they adopted and the characteristics of the population they studied. Another important finding from this work is that severe ED was commonest (61.7%) among the type 2 diabetic subjects with ED, followed by mild ED (26.7%) and moderate ED (11.7%). While moderate ED (66.7%) was commonest among the non-diabetic controls. This finding is similar to that of Ugwu et al [15]. Severe ED was commonest among his T2DM subjects (33.6%), followed by mild ED (19.1%) and lastly moderate ED (18.4%).
The prevalence rate of ED in patients with type 1 DM was 26% and 37% respectively [17, 18]. These two prevalence rates are close to that from this study and is far less than those from other studies that did not exclude hypogonadal type 2 DM patients. Hypogonadism is commoner in men with type 2 DM compared to those with type 1 DM largely because obesity is more in type 2 diabetes patients [38].
Correlation of IIEF scores with mean testicular volume, serum testosterone, and FSH and LH concentrations among type 2 diabetic subjects.
This study showed that there was positive correlation between the mean testicular volume and the IIEF score in type 2 diabetic subjects. There was also a positive correlation between serum testosterone level and IIEF score, although this was not statistically significant. The International Index of Erectile Function score on the other hand had negative, non-significant correlation with FSH and LH. This means that both the mean testicular volume and serum testosterone levels expectedly decreased with decreasing IIEF score. This agrees with the finding of Ugwu et al [15], that testosterone deficiency was significantly associated with erectile dysfunction in type 2 diabetic subjects.
From this study also FSH and LH increased with a decreasing IIEF score giving a biochemical picture of “hypergonadotropic eugonadism”. El Saghier et al found normal FSH and LH and low serum testosterone level (hypogonadotropic hypogonadism) in Egyptian type 2 diabetic subjects while Talukder et al found that low FSH and LH (hypogonadotropic hypogonadism) was commoner among Bangladesh men with type 2 DM and hypogonadism [39,40]. The above two studies unlike the index study evaluated type 2 diabetic subjects with low serum testosterone level.
The finding of decreasing testicular volume with decreasing IIEF score in this study agrees with that of Talukder et al that testicular volume was significantly lower in hypogonadal men with type 2 DM compared to their eugonadal counterparts [40].
The prevalence of erectile dysfunction in type 2 DM patients in Nnewi, south-eastern Nigeria is 48.4%.
The prevalence of ED in males with type 2 diabetes mellitus is about eighteen times higher when compared with their counterparts without diabetes mellitus.
There is significant positive correlation between IIEF scores and mean testicular volumes in the subjects with type 2 diabetes mellitus.
There is an urgent need for a routine screening for, early diagnosis of and prompt treatment of ED in type 2 diabetic subjects.
Recommendations
In view of the high prevalence of ED in type 2 DM patients in this study, it is recommended that, physicians and other health care professionals who treat diabetic patients would look out for ED and other chronic complications of DM in our diabetic patients routinely and take appropriate measures to tackle them.
In view of the wide variation in the prevalence of ED in subjects with type 2 DM from various studies, more studies on this very important and common complication of diabetes are needed to resolve this.
Limitations of the study
International Index of Erectile Function (IIEF) questionnaire that was used in this study is a self-report diagnostic tool. Its interpretation to the patients who do not understand English language may have reduced the accuracy of the responses given.
The Hospital Anxiety and Depression Scale questionnaire also used in the study is a self- report diagnostic tool. Its interpretation to the patients who do not understand English language as well as the socio-cultural implications of some of the questions in our setting could make some of the responses very subjective.
Elderly type 2 DM subjects were also enrolled and participated in this study and aging is a known risk factor for erectile dysfunction.
Patients who had both type 2 DM and hypertension, were included in the study because their exclusion would have limited the number of subjects for the study. These patients were either on angiotensin receptor blockers (ARBs), angiotensin converting enzyme inhibitors (ACE-Is) and or calcium channel blockers (CCBs). ARBs exhibit a beneficial effect on erectile function, while ACE-Is and CCBs have neutral effect.
Most of our study subjects who smoked tobacco or consumed alcohol had quitted prior to the commencement of this study mainly due to medical advice. The few subjects who still smoked tobacco and drank alcohol as at the time of the study may have influenced the outcome of this study because current smoking and heavy alcohol consumption were found to be associated with erectile dysfunction in both the diabetic subjects and in the general population.
Conflict of interest
The authors have no competing interest.
Funding
The authors did not receive any financial assistance for the research.
Abbreviation:
ED: Erectile Dysfunction; T2DM: Type 2 Diabetes Mellitus; HADS: Hospital Anxiety and Depression Scale; IIEF: International Index of Erectile Function; FSH: Follicle Stimulating Hormone; LH: Luteinizing hormone, PDE5: Phosphodiesterase type 5, cGMP: Cyclic guanosine monophosphate: ARBs: Angiotensin receptor blockers, ACE-Is: Angiotensin converting enzyme inhibitors, CCBs: Calcium channel blockers,
APPENDIX 1
HOSPITAL ANXIETY AND DEPRESSION SCALE (HADS)
This questionnaire has been designed to help you explain to your clinicians how you have been feeling.
Read each item below and indicate which comes closest to how you have been feeling in the past week. Ignore the numbers printed at the side. Don’t take too long over your replies; your immediate reaction to each item will probably be more accurate than a long, thought-out response.
DEPRESSION SCALE
A. Still enjoying the things i used to enjoy:
0- Definitely as much
1- Not quite so much now
2- Only a little
3- Hardly at all
B. I can laugh and see the funny side of things:
0- As much as I always could
1- Not quite so much now
2- Definitely not so much now
3- Not at all
C. I feel cheerful:
0- most of the time
1- Some times
2- Not often
3-Never
D. I feel as if I am slowed down:
0- Not at all
1- Sometimes
2- Very often
3- Nearly all the time
E. I have lost interest in my appearance:
0- I take just as much care as ever
1- I may not take quite as much care
2- I don’t take as much care as I should
3- Definitely
F. I look forward with enjoyment to things:
0- As much as I ever did
1- Rather less than I used to
2- Definitely less than I used to
3- Hardly at all
G. I can enjoy a good book or radio or television programme:
0- Often
1- Sometimes
2- Not often
3- Seldom
TOTAL SCORING:
<8>
>8= Depression
ANXIETY SCALE
A. I feel tense or “wound up”:
0- Not at all
1- From time to time, occasionally
2- A lot of the time
3- Most of the time
B. I get a sort of frightened feeling as if something awful is about to happen:
0- Not at all
1- A little but it doesn’t worry me
2- Yes, but not too badly
3- Very definitely and quite badly
C. Worry thoughts go through my mind:
0- Only occasionally
1- From time to time but not too often
2- A lot of the time
3- A great deal of the time
D. I can sit at ease and feel relaxed:
0- Definitely
1- Usually
2- Not often
3- Not at all
E. I get a sort of frightened feeling like ‘butterflies’ in the stomach:
0- Not at all
1- Occasionally
2- Quite often
3- Very often
F. I feel restless as if I have to be on the move:
0- Not at all
1- Not very much
2- Quite a lot
3- Very much indeed
G. I get sudden feeling of panic:
0- Not at all
1- Not very often
2- Quite often
3- Very often indeed
TOTAL SCORE:
<8>
>8= Anxiety
APPENDIX 2
INDIVIDUAL ITEMS FROM THE INTERNATIONAL INDEX OF ERECTILE
FUNCTION (IIEF) QUESTIONNAIRE AND RESPONSE OPTIONS
Circle the most appropriate Response option for each question
Question Response options
(All questions are preceded by “Over the past 4 weeks”)
1. How often were you able to get an erection during sexual activity?
0 No sexual activity
1 Almost never/never
2 A few times (much less than half the time)
3 Sometimes (about half the time)
4 Most times (much more than half the time)
5 Almost always/always
2. When you had erections with sexual stimulation, how often were your erections hard enough for penetration?
0 No sexual activity
1 Almost never/never
2 A few times (much less than half the time)
3 Sometimes (about half the time)
4 Most times (much more than half the time)
5 Almost always/always
3. When you attempted sexual intercourse, how often were you able to penetrate (enter) your partner?
0 Did not attempt intercourse
1 Almost never/never
2 A few times (much less than half the time)
3 Sometimes (about half the time)
4 Most times (much more than half the time)
5 Almost always/always
4. During sexual intercourse, how often were you able to maintain your erection after you had penetrated (entered) your partner?
0 Did not attempt intercourse
1 Almost never/never
2 A few times (much less than half the time)
3 Sometimes (about half the time)
4 Most times (much more than half the time)
5 Almost always/always
5. During sexual intercourse, how difficult was it to maintain your erection to completion of intercourse?
0 Did not attempt intercourse
1 Extremely difficult
2 Very difficult
3 Difficult
4 Slightly difficult
5 Not difficult
6. How many times have you attempted sexual intercourse?
0 No attempts
1 One to two attempts
2 Three to four attempts
3 Five to six attempts
4 Seven to ten attempts
5 Eleven + attempts
7. When you attempted sexual intercourse, how often was it satisfactory for you?
0 Did not attempt intercourse
1 Almost never/never
2 A few times (much less than half the time)
3 Sometimes (about half the time)
4 Most times (much more than half the time)
5 Almost always/always
8. How much have you enjoyed sexual intercourse?
0 No intercourse
1 No enjoyment
2 Not very enjoyable
3 Fairly enjoyable
4 Highly enjoyable
5 Very highly enjoyable
9. When you had sexual stimulation or intercourse, how often did you ejaculate?
0 No sexual stimulation/intercourse
1 Almost never/never
2 A few times (much less than half the time)
3 Sometimes (about half the time)
4 Most times (much more than half the time)
5 Almost always/always
10. When you had sexual stimulation or intercourse, how often did you have the feeling of orgasm or climax?
1 Almost never/never
2 = A few times (much less than half the time)
3 = Sometimes (about half the time)
4 =Most times (much more than half the time)
5 = Almost always/always
11. How often have you felt sexual desire?
1 = Very low/none at all
2 = Low
3 = Moderate
4 = High
5 = Very high
12. How would you rate your level of sexual desire?
1 = Very dissatisfied
2 = Moderately dissatisfied
3 = About equally satisfied and dissatisfied
4 = Moderately satisfied
5 = Very satisfied
13. How satisfied have you been with your overall sex life?
1 = Very low
2 = Low
3 = Moderate
4 = High
5 = Very high
14. How satisfied have you been with your sexual relationship with your partner?
I = Very low
2 = Low
3 = Moderate
4 = High
5 = Very high
15. How do you rate your confidence that you could get and keep an erection?
1 = Very low
2 = Low
3 = Moderate
4 = High
5 = Very high
TOTAL SCORE= ………………………………………..
No ED = Score of > 26
ED = Score of < 25>
Mild ED = 17-25
Moderate ED = 11-16
Severe ED = 6-10
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
